I think you know of the meaning of 'Neuro' in this word. Then, what does 'placiticity' mean ? Following is definitions of 'placiticity' from a few web dictionaries.
- the quality of being easily shaped or molded.
- the quality of being soft enough to be changed into a new shape
- the quality or state of being plastic
Extending this definition of 'placiticity' to the term 'neuroplaciticity', you may come up with your own definition for the term. Among the many different definition I can google, following seems to be one of the best described one to me. It is the definition from Britanica written as below.
Neuroplaciticity is the capacity of neurons and neural networks in the brain to change their connections and behaviour in response to new information, sensory stimulation, development, damage, or dysfunction.
Even without this kind of formal/dry definition, if you think of 'plastic' comparing to the hard materials like rocks, steel etc, you may have some intuition poping up in your mind, that intuition (whatever it is) would be the right definition.
Neuroplacity is the process or capability by which a neuron or a circuit of neuron 'changes' to perform various functions. This placiticity can be considered at various different levels. Sometimes it would indicates a specific part within single neuron (e.g, change of the numbers or forms of synapses), sometimes it may indicates the certain neural pathways which are involving huge amount of neurons and other supporting cells.
In early days of neuroscience research, we thought that our nerveous system gets fixed once we passed a certain developmental phase (i.e, a certain age in our life) but with recent researches we have been getting more and more evidence that our nerveous system is not that solid / fixed system and it continue to change to create new functions (e.g, learn new things and skills) and in some cases it changes its pathways to compensate the regions that had been damaged.
- Lifetime plan for development
- Good News and Bad News
- How neuroplaticity works ?
- Long Term Potentiation (LTP)
- Long Term Depression (LTD)
- Denervation supersensitivity
- Synaptic Strengthening
- Synaptic Pruning
- Adult neurogenesis
- Equipotentiality
- Vicariation
- Diaschisis
- Nature of Neuroplacitity
- How plasticity varies on Age
- Neuroplaciticy continues in life time
- Neuroplaciticy is NOT the cure for all
- Examples of Neuroplaciticity
- Structural changes in Hippocampi of Taxi Driver
- Second Language Aquisition
- Compenstation of Visual Impairment
- Brain Changes with Braille Learning
- Cheryl Schiltz' case
- A six-year-old boy's case
- Mora's case
- Is any region or neural path more plastic than others ?
- Is any region or neural path less plastic than others ?
Lifetime plan for development
Before I dive into the details of Neuroplaciticity, I want to introduce you an interesting plot that I got from a World Science Festival YouTube video.
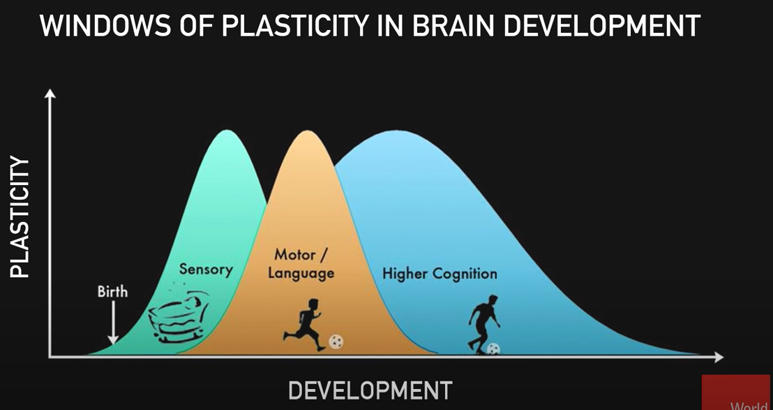
Image Source : The Nuts and Bolts of Better Brains: Harnessing the Power of Neuroplasticity - World Science Festival
As implied in the plot, there are a few points to note
- At the time of birth, the development of our brain is far from being complete. We are born with bare minimume of brain development
- Most of high level brain development occurs for very long period after birth. What's happening at the level of neuron changes and pathway changes happening in this period can be good topics for neuroplaciticity because neruons, its synaptic link with neighbouring neuron and forming / enhancing various neural pathways.
- Even though brain system for Sensory and Motor/Language completes relatively early stages in our life span, higher level cognitive function start developing from birth and continue to develop almost throughout the whole life.
Good News and Bad News
This is to set a proper expectation about the neurotransmitter. I don't like you to have too much expectation or too much disappointment,
There is both good news and bad news about the neuroplaciticity. When I was learning about nervous system (almost 40 years ago/1980s), it was generally believed that nervous system (especially the nervous system in higher animal) stops development only upto a certain age. So if you have any damages in nervous system after a specific age, it can never be recovered. However more and more researches shows that it is not the case. Those research shows that the nerve system development is an ongoing process spanning almost whole period of our life and can heal many types of the damages in various different ways. This is obviously a Good News.
However, you'd better not expect too much about this capability. The new development of nervous system does not work for every regions of nervous system. There are some part or functions of the nervous system that cannot be recovered once it get damaged. This is a bad news (at least not a good news). In addition, the capability of neuroplaciticity varies (usually get weaker) as we ages. This is definitely a bad news for the aging people including me.
How neuroplaticity works ?
Now let's look into the details of how neuroplaciticiy works (i.e, the mechanism of neuroplaciticity). Roughly speaking the neuroplaciticity happens at the two different level, structural and functional level. However, the border line between function and structural placiticity is not always clear cut. For example, if a neuroplacity happens by enhancing the synaptic connectibity between presynapse and post synapse and this enhancement happens by putting more neurotransmitter receptors on the cell membrane of the postsynaptic neuron, would you call this as a functional level placiticity ? or structural level placiticity ? You may call it as structural level placiticity if you observe cell membrane structure, but you may call it as functional level placiticity if you just observe electrical relationship between presynapse and post synapse without looking into the micro structural changes. So you may see a little bit of different categorization of functional and structural placiticiy depending on which text / articles you read.
Regardless of whether you call it as structural or functional, I would suggest you to get familiar with basic terminology for individual mechanism. I think Long Term Potentiation, Long Term Depression and Synaptic Pruning would be what you may hear or read from almost every text or videos/lectures dealing with neuroplaciticity.
Long Term Potentiation (LTP)
Long Term Potentiation is a phenomena where a synaptic response gets higher than regular cases when the same synapse is stimulated repeatedly. This is considered as the most fundamental phenomena for synaptic placiticity. It is often interprested as the first step for momory formation.
There are so many researches and evidences showing LTP and now would be one of the best established facts about synaptic placiticy (especially related to memory formation). One of the research/evidence is shown below. This experiment is done with neurons in Hipocampus.
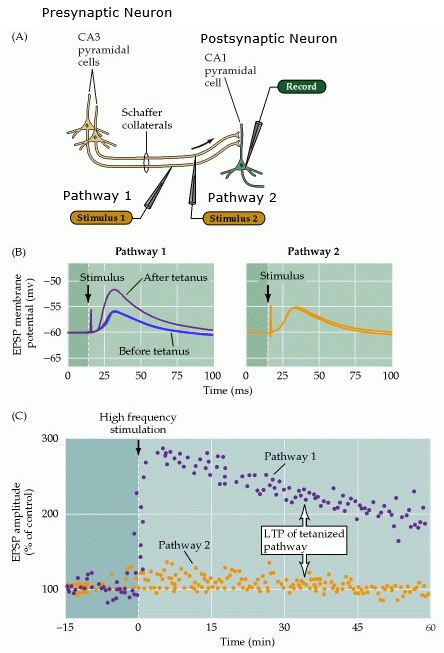
Image Source : Long-Term Synaptic Potentiation
[A] shows the illustration of test setup. You see the two pathways : Pathway 1 and Pathay 2. In these pathways, two different neuronal axons are stimulated by stimulus electrode : Stimulus 1 and Stimuls 2. The researcher used the two pathways for the comparative purpose. Pathway 1 shows long term potentiation and Pathway 2 does not. Before the measurement shown in the graph, the presynaptic neuron in Pathway 1 was stimulated multiple times (a high frequency sequence of stimulus pulse from Stimulus 1 electrode) and the presynaptic neuron in Pathway 2 was not stimulated.
[B] Shows the comparative plots measured at 'Record' electrode (post synaptic cell) when the same size of stimulus is applied by stimulus 1 and stimulus 2. As you may notice, The response for Pathway 1 (the pathway stimulated before the test) is much stronger than the case of Pathway 2 (the pathway with no previous stimulus).
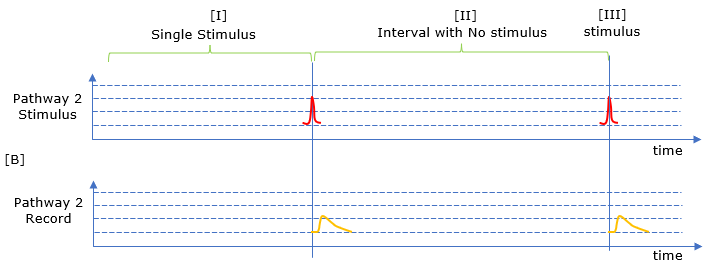
Following is the my own illustration of LTP. I hope this would better illustrate the concept.
< Synaptic response with LTP >
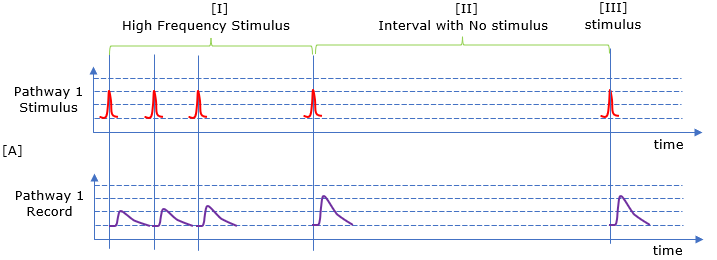
< Synaptic response with NO LTP >
NOTE : This video shows very clearly on how LTP is tested and measured : What Memories Are Made Of
There are many other examples of neuronal pathways showing LTP. As you may notice, most of them are from Hippocampus (CA), Sensory system (visual and auditory system). This is from a paper in 2004 and I am pretty sure that much more diverse cases has been researched by now.
< Pathways support LTP >
: The source of this list is [ Long-Term Potentiation and Memory - PHYSIOLOGICAL REVIEWS - 2004]
- Auditory thalamus → amygdala
- Entorhinal cortex → dentate gyrus
- Mossy fibers → CA3
- Commissural fibers → CA3
- Schaffer collaterals → CA1
- Hippocampus (CA1) → subiculum
- Hippocampus (CA1) → prefrontal cortex
- Subiculum → prefrontal cortex
- Thalamus → layer IV cortex
- Mesocortical thalamic nucleus → medial prefrontal cortex
- Cortico-cortical pathways
- Layer I → layer V
- Layer II → layer V
- Layer II/III → layer IV
- Cortex → striatum
- Dorsolateral geniculate nucleus → visual cortex
- Parallel fiber → Purkinje neuron
Long Term Depression (LTD)
Long Term Depression is a kind of opposite concept of LTP explained in previous section. In the synapse showing LTD, if you apply a sequence of stimulus at a presynaptic neuron, the potential measured at the post synpatic cell get smaller as shown in the following plot.
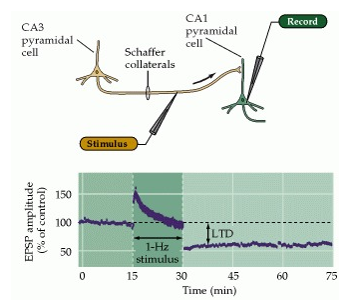
The potential shown in 0~15 min indicates the reference potential measured at the 'record' electrode. The range shows the meaured potential when a sequence of consecutive stimulus (once per second). As you see, the response is gradually decreases. And the with a brief break, stimulus is applied and the measured reponse (measured voltage) gets much lower than normal as shown in the range from 30 and later.
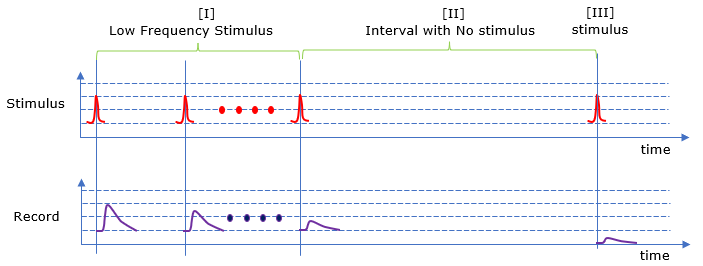
Following is my own representation of the concept of LDP. I hope this would be easier for me to understand.
Denervation supersensitivity
As you may notice from the terminology, it is about the fact that some neuron get supersensitive (to the same input signal). Why do they become supersensitive ? It happens when some of corticol neurons are lost. Due to this neuron loss, a signal path to which the lost neuro used to belong gets disconnected(i.e, denervated). In order to compensate this, the post-synaptic membrane develop more receptors for neurotransmitters leading to super sensitivity for the post synaptic neuron (refer to this article).
- This was reported to a skeletal muscle which lost some of nuerons connected to the muscle fiber (see this paper)
- This doesn't mean that any kind of neuronal damage can be compenstated by the supersensitivity. If the amount of the damage is greater than a certain range, the neural path would get contracted which is called degenerative contranction (see this paper).
Synaptic Strengthening
Synaptic strength is an indicator showing how strong potential (voltage or current) at post synaptic neuron when a stimulus is applied to the presynaptic neuron. You may take it as the ratio of output to input. For example, in LTP you can say the synaptic strength got increased and in LTD you can say the synaptic strength got decreased.
Synaptic Strengthening is any mechanism (or structural change) that increase the synaptic strength.
Synaptic Pruning
In gardening (horticulture), pruning means cutting off (trimming) unused/not-useful branches. Same applies to Synaptic Pruning. Synaptic Pruning means removing synapses which are not used.
This usually observed in some part of mammalian brain during the early stage of brain development. As shown in the image below, the number of synapsis continuosly increases from embryonic stages through a certain ages. But from a certain ages, only those synapsis which recieves stimulus remains and others (non-used) synapses gets removed (i.e, gets pruned).
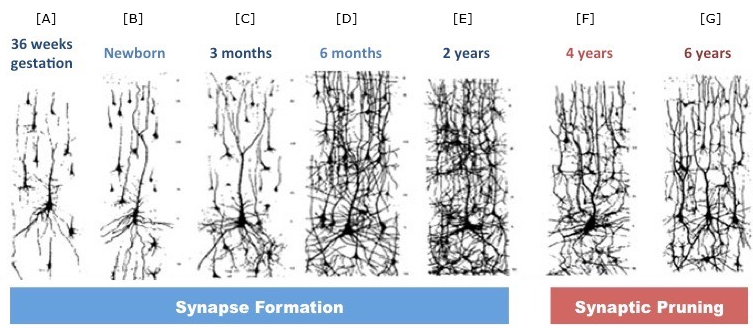
Image Source : Synaptic Formation - BioNinja
< Examples of Synaptic Pruning >
Follwoings are some of the examples of synaptic prunning.
- Early emborynic stage to 2 years : New neurons and synapses are formed at an extremely high rate
- Ages 2 to 10 years : the number of synapses drops dramatically (i.e, synaptic pruning happens rapidly)
- Adolescence : Synaptic pruning continues but not as fast as before
- Early adulthood : Synaptic pruning continues mostly in the prefrontal cortex of the brain and seems to stop in the late 20s
< Medical conditions associated with Pruning >
There some medical conditions associated with unusual level of synaptic pruning. Followings are some of the examples even though most of these conditions and its association with synaptic prunning is at still early stages of research.
Brains of individuals with schizophrenia, for example, have fewer synapses than normal. Some researchers have hypothesized that excess synaptic pruning could trigger the diseaselikely during the active period of synapse elimination in adolescence, which coincides with the typical onset of schizophrenia.(How synaptic pruning shapes neural wiring during development and, possibly, in disease).
Note : Even though over pruning is observed in cortex of the brain of schizophrenia, some research shows that a specific part of hippocampus shows more dendritic spikes in schizonphrenia patient than control group (Discovering Neurobiology for Psychosis)
Note : Under-pruning may imply that higher connectivity. But this can be observed differently (in some case observed contradictory) based on various factors like 'local vs global' brain region or developmental stages etc (Network Neuroscience of Autism)
Adult neurogenesis
Neurogenesis is a process of generating new functional neurons from precursor cells. So 'Adult Neurogenesis' is a processing of generating new functional neurons from 'adult' precursor cells. Why 'Adult Neurogensis' is so sopecial ? It is because it had long been thought that this kinds of neurogenesis happens only in emborionic or prenatal stages in higher animal like mammalian. But recent study shows that this kind of neurogenesis happens throughout the whole life in some restricted area of nervous system (Note the keyword 'restricted area' meaning that unfortunately not every area of nervous system can undergo neurogenesis when it reaches a certain point in life).
Since the first evidence of adult neurogenesis in Hippocampus of a rat brain, many other cases of adult neurogenesis was observed among various animals (refer to this paper)
Equipotentiality
Equipotentiality is a capacity of neural system in which normal functioning part (intact part) of the system to carry out the functionality of a damaged part to make the overall neural system function as normal. This theory was postulated at early memory research. Some scientists make small lesions on various locations of brain (rat brain) and check if the lesion cause any memory loss. The result showed that those small lesions (damages) does not cause any visible problems wherever you make unless the amount of the legion (damage) reaches considerably large area. This result lead to a few hypothesis as follows.
- Memory is not localized, it is globally distrubed all over the brain. ==> This hypothesis was contradicted by the case of H.M and others shows that a certain part of the brain region (localized region) cause serious memory loss / memory formation.
- The functionality of a damaged part can be compensated by the intact part to make overall functionality work normally. This is the theory of Equipontentiality. I saw some of the papers supporting this theory, but I am not sure if this theory has been accepted as a well established fact or not.
I want to introduce a little bit different way of defining Equipotentiality which is defined in What is Neuroplasticity? A Simplified Guide as follows : (I personally like this definition since it fits better for the term 'equal' in the term equipotentiality.
Vicariation
Vicariation sounds mouthfull to me and I have no idea on what it would literally mean. Even googling I haven't find any definition that sounds clear to me. One of the definition that I think is best fit for me is :
Still not so clear to me. In other words, Vacriation refers to the process by which one brain area or system can compensate for the loss or damage of another brain area or system. I think it would be clearer if I see some cases of examples as listed below. I got these examples from chatGPT.
- After a stroke, an individual may experience paralysis on one side of their body. In response, the brain may compensate by increasing the strength of connections between the undamaged brain areas that control the non-paralyzed side of the body. This can allow the individual to regain some degree of control over their movements.
- After a traumatic brain injury, an individual may experience problems with memory and learning. In response, the brain may develop new connections between brain areas that are involved in these functions, allowing the individual to compensate for the damaged areas.
- In individuals with hearing loss, the brain may compensate by increasing the strength of connections between brain areas that are involved in processing visual information, such as from sign language or lip reading. This can allow the individual to maintain or improve their communication abilities.
- In individuals with vision loss, the brain may compensate by increasing the strength of connections between brain areas that are involved in processing auditory and tactile information. This can allow the individual to maintain or improve their ability to navigate and interact with the world.
Diaschisis
Diaschisis refers to a temporary decrease in function of a particular brain region as a result of damage or injury to a connected area. As mentioned, Diaschisis is usually temporary symptom and it gradually recover to normal in most cases. For now, exact mechanism behind Diachisis is largely in mystery and require further researches, it is believed that synaptic changes or neurotransmitters are involved in this symptom.
There are some examples of Diaschsis as follows.
- Temporary decrease of a brain functions after stroke : This can result in a variety of symptoms, such as weakness or paralysis on one side of the body, difficulty speaking or understanding language, and changes in vision or other sensory functions. This symptom may recover to normal as the decreased functionality is recovered directly or other brain area start compensating the decreased functionalities.
- Temporary descrease of a brain function after brain surgery (e.g, removing brain tumer) : The regions around the removed part (the tumor region) may suffer from the decrease of function. This can lead to changes in cognitive function, such as difficulty with memory or attention, as well as changes in sensory or motor function
- Temporary descrease of a brain function after concussion : You may suffer from a temporary decrease in function, leading to symptoms such as headache, dizziness, and difficulty with memory and concentration. But in most case you would recover to normal as time goes on.
Nature of Neuroplacitity
How plasticity varies on Age
In general, neuroplaciticity occurs more actively in young ages, especially within a few years after the birth.
Neuroplaciticy continues in life time
Even though neuroplaciticiy happens more actively in young ages in general, it happens throughout the whole life.
Especially the neurons involved in learning, experience, and memory formation would happen relatively actively even in adult ages.
In some cases when a part of brain is damaged (e.g, stroke), healthy part of the brain would take over the functionality of the damaged part.
Neuroplaciticy is NOT the cure for all
Even though Neuroplaciticy is ongoing process throughout lifetime and some of damaged part can be compensated by some other part of the brain, it is important to know that neuroplaciticity is not a solution for every problem. You should consider the possible restriction of neuroplaciticity as follows :
- Some part of the brain does not show the placiticity
- Even though some damage can be compensated by other part of the brain, the damage may not get fully recovered if the scope of the damage is very wide.
Examples of Neuroplaciticity
There has been wide range of researchs about neuroplaciticy. In this section, I want to introduce some of the most popular (widely mentioned in many lectures) examples of these researches.
Structural changes in Hippocampi of Taxi Driver
This would be an example that are most frequently mentioned in lectures and videos as an evidence showing that neuroplaciticity really happens. It is about the research from London Taxi driver. Comparing to other jobs, Taxi driver would use more of the brain parts that are associated with figuring out geographical maps and memories about those facts.
The conclusion of this research can be summarized as below : (If you are interested in further details, check out the original paper linked at the bottom of the image).
- There are not meaningful difference in terms of overall volumn of Hippocampus
- posterior part of Hippocampus of those taxi drivers are developed more than others (control group). ==> Since there is no significant difference in overall volumn of hippocampus, this indicates some other parts of the Hippocampus of taxi driver would be smaller than control group. In conclusion, anterior part of Hippocampus of taxi driver is smaller than the case of control group.
- the degree of development of posterior Hippocampus of the taxi driver gets higher as their experience as taxi driver gets longer
The subjects in this research are as follows. One thing you may notice is that all of them are adults with a few years of experience as a taxi driver. This would be a good indicator that the placiticity happens even during the adulthood
- mean age 44 years; range 3262 years
- licensed London taxi drivers for more than 1.5 years
- The average time spent training to be a taxi driver before passing the licensing tests fully (i.e., time on The Knowledge) was 2 years
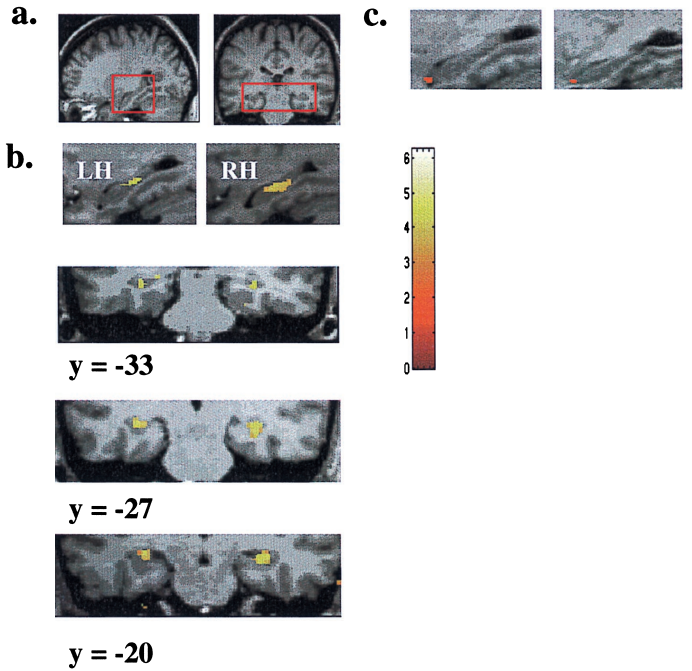
The brain image evidence showing that the taxi driver shows higher development in a specific area of Hippocampus is as follows.
- Significantly increased gray matter volume was found in the brains of taxi drivers compared with those of controls in only two brain regions, namely the right and the left hippocampi as shown in a and b.
- No differences were observed elsewhere in the brain.
- The increase in hippocampal gray matter volume was focal and limited to the posterior hippocampus bilaterally
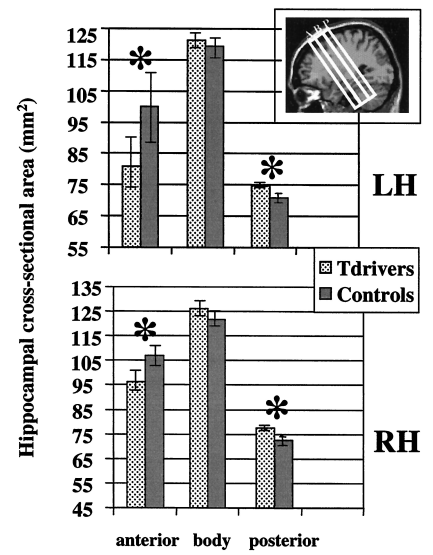
Following plot shows the volumn changes of three different parts of Hippocampus of taxi drivers. It can be summarized as below :
- Anterior part of Hippocampus : In this area, the volumn size in taxi driver is smaller than the control group. The difference is even greater in the hippocampus in left hemisphere comparing to the case of right hemisphere.
- Body part of Hippocampus : There are small difference between taxi driver and control group, but not much meanigfully different.
- Posterior part of Hippocampus : The volum size of the hippocampus in tax driver is larger than the case of control group. ==> absolute different may not look such a big difference comparing to the body part, but if you take the ratio of the difference it is greater (statistically meaningful) than the case of the body part.
Following plot shows the correlation between the volum increase of posterior Hippocampus and the length of experience month of tax drivers. The conclusion is that the volum of posterial Hippocampus increases over time whereas the anterial Hippocampus volume decreases over time.
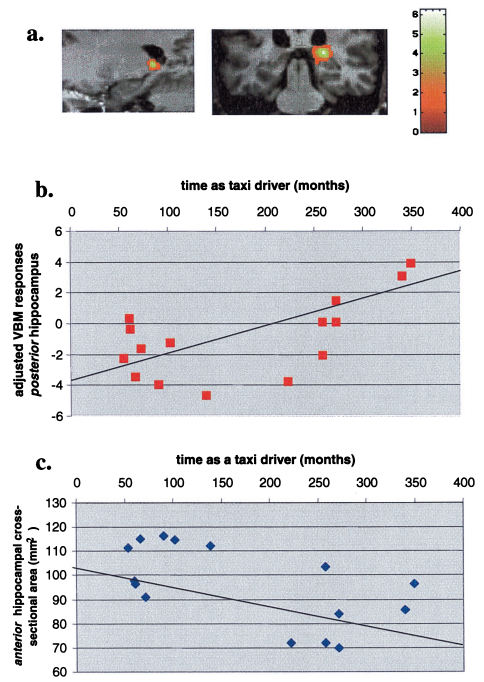
Image Source : Navigation-related structural change in the hippocampi of taxi drivers - PNAS (2000)
Second Language Aquisition
First language acquisition (learning the mother tungue) is intrinsic part of the brain and the development for this would be done for almost everybody, but the second langauge aquision is mostly done by active learning.
The pioneering research on this area was published in Nature in 2004 as stated below :
NOTE : Grey matter is the part formed by bundles of cell body parts of neurons. High density of Grey matter would imply the more number of cell body or more synaptic connections among neurons.
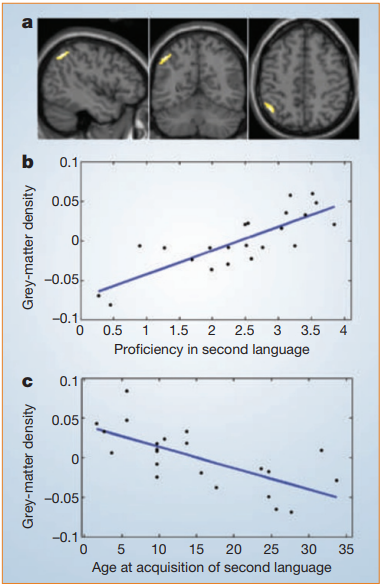
Image Source : Structural plasticity in the bilingual brain - Nature (2004)
[a] shows the location of brain area that shows the increased grey matter density from the aquision of the second language.
[b] shows the relationship between the preficiency in second language and Gray matter density. You would notice that the grey matter density increases as the proficiency of the second languate (i.e, gray matter density is proportional to the proficiency in the second language)
[c] shows the relationship between the age at the acquisition of the second language and Gray matter density. You would notice that the earliear you learn the second language, the higher grey matter density is (i.e, gray matter density is anti-proportional to the the age at the aquision of the second language)
Compenstation of Visual Impairment
This paper shows the case of neuroplaciticity where visual cortex area of those persons who has vision imparment. In these patient, the visual cortex would not process visual information/stimulus since they are visually impaired. Then the area for the visual cortex remain unused at all for those patients ? According to this review paper, the area of visual cortex still active but it mainly used for processing other sensory inputs instead of processing visual input.
Following image shows how the visual cortex are of the visually impared person are utilized for other purpose. Pay attention to color code when you compare each of the image (A,B,C). [A] shows the cortex area for visual processing in Healthy person. [B] shows the area that are involved in language comprehension and semantic processed. [C] shows the cortex functionality in Visually Impaired person. You would notice that large prtions of visual cortex is replaced by green and blue colors indicating language comprehension and semantic processes and the yellow/orange are shrinked greatly.
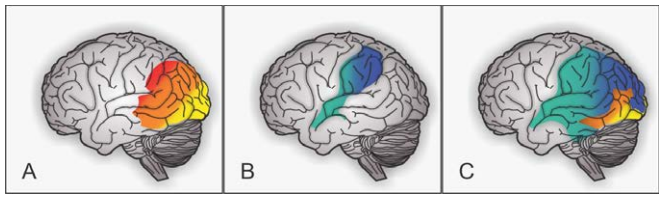
Image Source : Neuroplasticity in visual impairments - Neurology International (2018)
Following image shows another aspect of how the visual cortex of the visually impared person are utilized for other purpose. [A] shows the case of visual cortex development in healthy indivisual. At the birth, the visual cortex would have synapsis not only for Vision processing but also for processing other inputs like hearing (audition), touch (Tact) and Smell (olfactory). Of course, the vision processing is main functionality of this cortex area but there are some of synapsis associated other functionality (e.g, hearing, touch, smell etc). As the individual experience various visual inputs after birth, synapsis for hearing / touch / smell gets inhibited and eventually get removed.
[B] shows the case of visual cortex development (placiticity) for the indivisuals with visual imparement. Since these individual does not get any visual stimulus, the synapses for vision processing would get degenerated (removed) and the remaining functionality (like hearing, touching, smell etc) would get more developed. Since the indivisuals with the impairment from the birth has more of the synapses for hearing, touching, smell comparing to the individual with the impairment at later age, the indivisuals with the imparment from the birth shows stronger placiticity (i.e, developing other functionality at the visual cortex) comparing to the other cases.
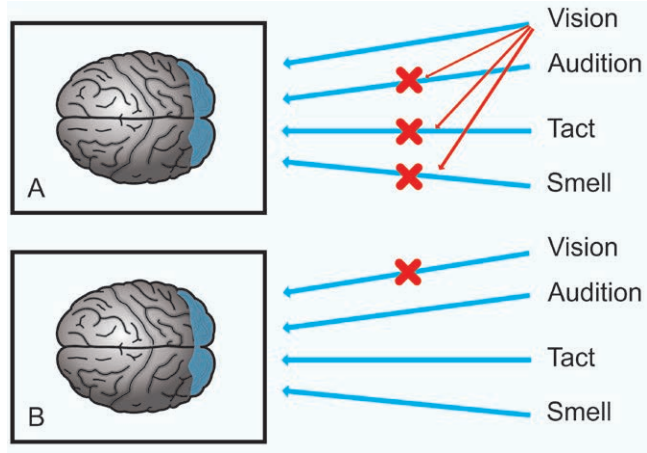
Image Source : Neuroplasticity in visual impairments - Neurology International (2018)
Some of the bullets that would give you a little bit further details from this papar are listed below :
The neural networks reorganization in neuroplasticity in blind patients is a compensatory form of visual deprivation, mainly with the increased sensitivity to touch, smell and hearing Cortical thickness is related to neuroplasticity, differently between congenital and late blind. the visual cortex of early blind are thicker than the late blind and non-blind. The congenital visual impairment has a greater cortical thickness in areas associated with vision, while those with late blind have little or no cortical surface reduction. ==> The reason why the peron with visual imparment at congenital period (i.e, at the time of birth) would be because they haven't gone through the process of eliminating non-functional synapses which is caused by visual input during the early developmental stages (especially 2-4 month after birth) in healthy individuals. ==> Since the indivisual with visual imparement at early stage has more (diverse) functional synapses, they shows increased placiticity comparing to those with the imparement at later ages.the occipital cortex participates in the tactile, auditory and olfactory functions improvement. brain plasticity depends on the age of vision loss and can occur basically in two ways: cross-plasticity and multimodal
Brain Changes with Braille Learning
This case investigates neuroplastic changes in sighted adults during an 8-month tactile Braille reading course. The study monitored brain structure and function at five different time points using MRI techniques. Key findings include adaptations in the reading network of the ventral occipitotemporal cortex to tactile input and changes in grey matter volume and intracortical myelin in sensory areas. These results contribute to understanding the neuroplastic mechanisms underlying complex cognitive systems and their sensory inputs and motor outputs.
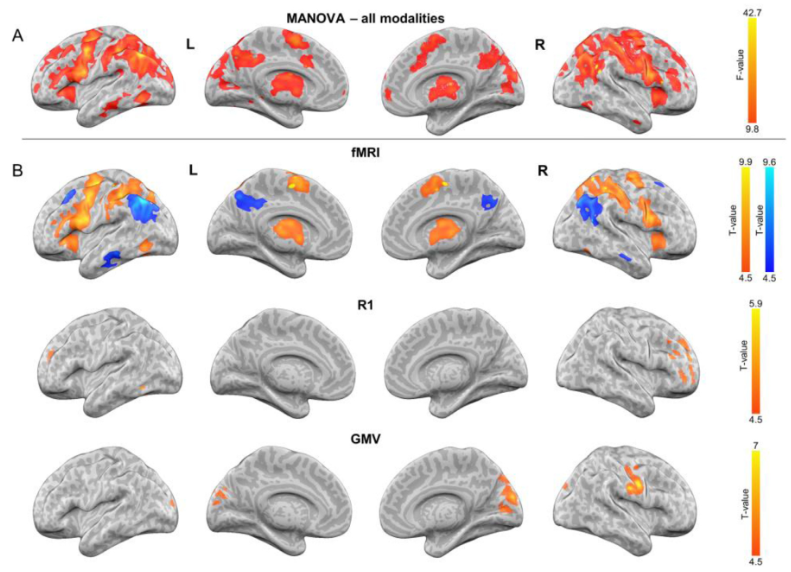
Image Source : Brain plasticity dynamics during tactile Braille learning in sighted subjects: Multi-contrast MRI approach - NeuroImage (2021)
Each type of scan provides different information about the brain. While fMRI is more about immediate functional changes, R1 and GMV provide insights into more structural and potentially long-term changes in the brain's anatomy. The difference in active areas between these scans underscores the multifaceted nature of brain plasticity, involving both functional and structural changes in different regions, depending on the type of learning and the sensory input involved.
MANOVA - all modalities: This panel is likely showing the results of a multivariate analysis of variance (MANOVA) across all modalities, which means it's looking at multiple outcomes across the different types of data collected (such as structural and functional MRI data). The areas highlighted in red probably indicate regions where there was a statistically significant change or difference observed over time or between groups.fMRI : This panel shows functional MRI (fMRI) results, which measure brain activity by detecting changes associated with blood flow. The orange and yellow areas indicate regions with increased activity, while blue areas indicate decreased activity, related to the tactile Braille reading task. The areas highlighted in the fMRI scans correspond to regions of increased neural activity during the tactile Braille reading task. These are dynamic changes that occur as the brain engages in a particular function.R1 : This could be a specific type of MRI contrast (possibly related to quantitative T1 mapping mentioned in the paper), which provides information about the physical properties of brain tissue. The areas in orange could indicate regions where there has been an increase in the parameter being measured, suggesting a change in brain tissue properties. The R1 image could be related to a quantitative MRI parameter, potentially representing the rate of longitudinal relaxation (T1) of brain tissue. Changes in R1 may reflect alterations in tissue properties that are not directly related to task-induced activity but could indicate longer-term structural changes such as myelination or other tissue composition alterations.GMV (Gray Matter Volume) : These images show changes in gray matter volume, with increases indicated by the warmer colors. An increase in gray matter volume in specific areas of the brain may be associated with learning and the formation of new neural connections. Increases in gray matter volume in certain brain areas can be associated with neuroplasticity, indicating structural changes that could be due to learning, the development of new skills, or the strengthening of neural connections.
- Problem Description: Cheryl Schiltz suffered from a drastic loss of balance due to damage to her vestibular system, caused by the antibiotic gentamicin. This condition left her with a constant sensation of falling, severely impacting her quality of life.
- Solution: To address this, her doctor devised a novel treatment involving a helmet with motion sensors. These sensors sent signals to a metal strip in her mouth, creating a new sensory feedback mechanism to aid in balance.
- Conclusion: This treatment exemplified the brain's neuroplasticity, as Schiltz gradually learned to interpret these signals for balance. It highlights the brain's ability to adapt and compensate for lost functions, significantly improving her balance and reducing her dependence on the device.
- Problem Description: A six-year-old boy had a brain tumor causing severe seizures, unresponsive to medication. The treatment required the removal of about a third of the right side of his brain, including the entire occipital cortex and most of the temporal lobe, crucial for basic sight functions.
- Observation: Post-surgery, the boy was closely monitored and assessed over three years. Functional brain scans showed that most visual functions, like face and object recognition, were taken over by the left side of the brain, demonstrating its capacity to reorganize.
- Conclusion: Despite losing significant brain tissue, the boy's cognitive functions and IQ (118 post-surgery compared to 116 pre-surgery) remained remarkably intact. This case underscores the brain's plasticity, especially in children, and its ability to adapt to even drastic changes in its structure. This case demonstrates the extraordinary adaptability of the young brain. Despite losing a large portion of the brain, which included areas critical for vision, the boy's cognitive development remained remarkably resilient. His brain compensated for the loss by reorganizing and reallocating functions to other areas, particularly the left side. This adaptability not only preserved but slightly enhanced his cognitive abilities, as reflected in a small increase in his IQ. This case highlights the remarkable potential of the brain to rewire and adapt, especially in younger individuals.
- Problem Description: Mora Leeb had a stroke before birth, leading to a damaged left brain hemisphere and severe epilepsy.
- Solution and Observation: At 9 months, she underwent a hemispherectomy, a drastic procedure that removed the left side of her brain. Post-surgery, Mora's right hemisphere began to take over functions typically managed by the left hemisphere, including speech and motor skills. Her progress was supported by extensive rehabilitation, including physical and speech therapy.
- Conclusion: Mora's recovery illustrates the young brain's incredible plasticity. Her ability to adapt and reorganize functions, typically located in the removed hemisphere, highlights the potential for neurological recovery and adaptation in early childhood.
Is any region or neural path more plastic than others ?
Seemingly Yes, but the answer may vary depending on situations or how you define the placitity. I think I need to read more articles or papers to have clearer understanding on this topic, but following is general idea that I have as of now.
- The
hippocampus is known for its remarkable capacity for plasticity and neurogenesis (the birth of new neurons). Studies have shown that the hippocampus can regenerate and restore some of its function even after significant damage or injury. - Similarly, the motor cortex has been shown to have a high degree of plasticity and potential for recovery after injury. Studies of stroke patients, for example, have shown that with intensive rehabilitation and training, the motor cortex can reorganize itself and recover lost function.
- In contrast, the
visual cortex and prefrontal cortex may have a lower probability of recovery after damage. The visual cortex is involved in processing visual information, and damage to this region can result in blindness or other visual impairments. While some degree of recovery is possible with rehabilitation and training, the visual cortex may be less capable of regeneration and restoration than the hippocampus or motor cortex. - Similarly, the
prefrontal cortex is involved in higher cognitive functions such as decision-making and working memory, and damage to this region can result in significant impairments in these abilities. While some degree of recovery is possible with rehabilitation and training, the prefrontal cortex may be less capable of regeneration and restoration than the hippocampus or motor cortex.
Is any region or neural path less plastic than others ?
Seemingly Yes, but as in previous section the answer may vary depending on situations or how you define the placitity. I think I need to read more articles or papers to have clearer understanding on this topic, but following is general idea that I have as of now.
It is considered that basal ganglia and primary auditary cortex is less plastic then others.
Basal ganglia is a group of structures deep within the brain that are involved in movement control, habit formation, and reward processing. While the basal ganglia can adapt to changes in the environment and experience, they may be less plastic than other brain regions, particularly in terms of generating new neurons.primary auditory cortex is involved in processing sound information. While the auditory cortex can adapt to changes in the environment and experience, it may be less plastic than other sensory regions, such as the visual cortex.
YouTube
- Memories that Last: Genes Neurons and Synapses - UCTV (2011)
- How synapses spark - MaxPlanckSociety (2012)
- After watching this, your brain will not be the same | Lara Boyd | TEDxVancouve (2015)
- Richard Huganir: Synaptic plasticity mechanisms underlying learning in the brain (2016)
- 4.4 Synaptic plasticity - Cellular Mechanisms of Brain Function (2016)
- Neuroplasticity: Our Adaptable Brain with Nick Spitzer - On Our Mind - UCTV (2017)
- Synaptic Plasticity - Neuroscience Online (2017)
- Neuroplasticity, Animation. (2018)
- Rewiring Revolution:Neuroplasticity's Impact on Wellbeing | Kristen Meisenheimer | TEDxSanLuisObispo (2019)
- Brain Plasticity: A Mental Health Renaissance | Hani Akasheh | TEDxPSUT (2019)
- The Nuts and Bolts of Better Brains: Harnessing the Power of Neuroplasticity - World Science Festival (2019)
- The Brain's Flexibility To Learn And Adapt In Childhood | The Brain Fitness Program - Spark (2019)
- What Happens To The Brain In Old Age? | The Brain Fitness Program | Spark - Spark (2019)
- How The Brain Affects Your Sight And Sound | The Brain Fitness Program | Spark - Spark (2019)
- Temporal and Spatial Summation - 10 Minute Phyaiology (2021)
- What Memories Are Made Of - BrainFacts.org (2021)
- How the Brain Responds to Blindness - Institute of Human Anatomy (2022)
- Re-wiring the Brain #science #brainpower #humanbody - Magellan (2025)
- Autism/Asperger/Savant
- Neurobiological changes in autism spectrum disorders-Holland Bloorview Kids Rehabilitation Hospital (2013)
- Communication difficulties in Aspergers - Kanti (2015)
- Asperger's 5 step thought process - Kanti (2015)
- Autism: An evolutionary perspective, Professor Simon Baron-Cohen, 1st Symposium of EPSIG - (2016)
- Autism: A view from neuroscience - A CCN public lecture - Dartmouth (2018)
- Update on Brain Research in Autism - UCLACART (2018)
- Genetics, Brain Connections and Autism - Inside Science (2020)
- Inside the autism brain: The striatum - Spectrum Autism Research News (2020)
- Network Neuroscience of Autism - Mailman Center for Child Development (2020)
- Schizophrenia
- What is Schizophrenia? - It's More Than Hallucinations - Dr.Tracey Marks (2019)
- Discovering Neurobiology for Psychosis - UCSF Dept. of Psychiatry and Behavioral Sciences (2021)
- Can Brain Scans and Imaging Help in Diagnosing Schizophrenia? | with Dr. Tracey Marks - Living Well with Schizophrenia (2022)
- Advanced Research
- Artificial embryos: the hidden steps in forming a spine - nature video (2022)
- Why Different Neuron Parts Learn Differently? - Artm Kirsanov (2025)
Reference
- neuroplasticity - Britannica
- Neuroplasticity - Physiopedia
- Neuroplasticity - EMOTIV
- Long-Term Synaptic Potentiation - NIH/National Library of Medicie
- Long-Term Synaptic Depression - NIH/National Library of Medicie
- Long-Term Potentiation and Memory - PHYSIOLOGICAL REVIEWS - 2004
- What Is Synaptic Pruning? - headline.com
- Synaptic Formation - BioNinja
- Denervation supersensitivity in skeletal muscle: analysis with a cloned cDNA probe - NIH/National Library of Medicine
- Equipotentiality - Wikipedia
- Equipotentiality of Thalamo-Amygdala and Thalamo-CorticoAmygdala Circuits in Auditory Fear Conditioning - The Journal of Neuroscience (1992)
- THE ONSET OF DENERVATION SUPERSENSITIVITY - ASPET/THE JOURNAL OF PHARMACOLOTY AND EXPERIMENTAL THERAPEUTICS (1966)
- Synaptic plasticity: Step-wise strengthening - Current Biology (1998)
- Navigation-related structural change in the hippocampi of taxi drivers - PNAS (2000)
- Structural plasticity in the bilingual brain - Nature (2004)
- Our flexible friend - The Guardian (2009)
- Adult Neurogenesis in the Mammalian Brain: Significant Answers and Significant Questions - NIH/National Library of Medicine (2011)
- The molecular biology of memory: cAMP, PKA, CRE, CREB-1, CREB-2, and CPEB - Molecular Brain (2012)
- Why Synaptic Pruning is Good - Gemm Learning (2013)
- Diaschisis - ScienceDirect (2014)
- Loss of mTOR-Dependent Macroautophagy Causes Autistic-like Synaptic Pruning Deficits - Neuron (2014)
- Dynamic Brains and the Changing Rules of Neuroplasticity: Implications for Learning and Recovery - Frontiers (2017)
- Why Is Synaptic Pruning Important for the Developing Brain? - Scientific Amearica (2017)
- What Is Neuroplasticity? A Psychologist Explains [+14 Tools] - PositivePsychology (2018)
- Neuroplasticity in visual impairments - Neurology International (2018)
- What Is Synaptic Pruning? - Healthline (2018)
- Boy loses huge brain section, his IQ goes up - COSMOS (2018)
- 6 Ways to Rewire Your Brain - healthline (2020)
- How synaptic pruning shapes neural wiring during development and, possibly, in disease - PNAS (2020)
- Brain Differences - emabrace autism (2021)
- Brain plasticity dynamics during tactile Braille learning in sighted subjects: Multi-contrast MRI approach - NeuroImage (2021)
- mTOR-related synaptic pathology causes autism spectrum disorder-associated functional hyperconnectivity - NIH/National Library of Medicine (2021)
- Neuroplasticity - NIH/National Library of Medicine (2022)
- What Is Neuroplasticity? - verywell mind (2022)
- What is Neuroplasticity? A Simplified Guide - Psychscene Hub (2022)
- What is Neuroplasticity? (Definition + Examples) - Practical Physiology (2022)
- Molecular mechanism of hippocampal long-term potentiation Towards multiscale understanding of learning and memory - Neuroscience Research (2022)
- Rewiring the Brain: The Promise and Peril of Neuroplasticity - World Science Festival (2023)
- Meet the 'glass-half-full girl' whose brain rewired after losing a hemisphere - npr (2023)
- Autism/Asperger/Savant
- Autism as a neural system disorder: A theory of frontal-posterior underconnectivity - NIH/National Library of Medicine (2004)
- Underconnected, but how? A survey of functional connectivity MRI studies in autism spectrum disorders - NIH/National Library of Medicine (2011)
- Brain connectivity and high functioning autism: a promising path of research that needs refined models, methodological convergence, and stronger behavioral links - NIH/National Library of Medicine (2012)
- Idiosyncratic connectivity in autism: Developmental and anatomical considerations - NIH/National Library of Medicine (2015)
- Synaptic growth, synesthesia & savant abilities - Embrace Autism (2021)
PodCast
- Neuroplasticity_Overview_01
- Neuroplasticity_Overview_02
- Neuroplasticity_KeyConcept_01
- Neuroplasticity_Definition_01
- Neuroplasticity_History_01
- Neuroplasticity_LevelOfPlaciticity_01
- Neuroplasticity_NatureOfPlaciticity_01
- Neuroplasticity_DifferenceByRegion_01
- Neuroplasticity_Examples_01